

During an interview for a feature in Allure Magazine, The primary aim of beautification surgery is to enhance attractiveness while maintaining a natural look. In planning surgery, my beautification approach often has effects that can positively impact the arc of aging (see Q9 re: the “trajectory of aging”). However, while age is a factor, anatomy is the primary driver.
1. How do you define it?
A “beautification facelift” (or “optimization facelift” as a gender-neutral term) enhances a face’s attractiveness towards an “aesthetic ideal,” whereas a rejuvenating facelift restores a face to a prior appearance that has shifted with the passage of time. While a youthful look can be a result of both, my approach to face optimization surgery targets the 4 psychological “beauty cues” to which humans are wired to respond: neoteny, symmetry, sexual dimorphism (features that conjure masculinity or femininity), and supra-averageness (think overall facial harmony). An “optimized” face looks natural yet induces the observer to resonate with beauty cues more intensely than the prior appearance — a subconscious effect. Surgical modification of anatomy to strike the right balance of these cues, and not overdoing one or the other, is the art, while patient goals and anatomy are the drivers, not simply age. (see Q4 for the “how”).
2. And what are you typically treating when aiming to “optimize” or “beautify” rather than “rejuvenate”?
See Figures 1 – 4 below.
Both surgical optimization and rejuvenation address soft tissue laxity (skin, fat, muscle and fascia), but my optimization approach uniquely targets disharmonies in 3 areas: bone structure, feature proportions and facial framing.
1. Bone structure:
Often, patients have had prior filler treatment for flat cheekbones and hollow under eyes. However, if underlying bone structure is lacking then fillers can unnaturally inflate — rather than support — tissues, and adding more weight over an unsupported framework only worsens droop. I often correct inadequately supported cheeks and under eyes with porous polyethylene implants, a biocompatible, permanent medical-grade bone-like material with microscopic pores that allow tissue and blood vessel ingrowth, helping to securely anchor them in place and to create natural-appearing facial contours.
2. Feature proportions:
Modifying specific facial features — eyes, lips, nose, jaw and chin — to improve their shape and make them appear larger or smaller can be beautifying. I use “direct” aesthetic effects — modifying the feature itself — and “indirect” effects — reducing the size and frame of the face to make the features look larger. (See Q4 for more detail on “direct” and “indirect”.)
3. Facial framing:
Modifying the outer frame for more harmonious length and width balance, and sculpting face shape, both can accentuate beauty cues. For example, a heart shape and gently curving face contour can set a female face to best advantage, whereas chiseling contours and squaring the jaw and chin can bring more masculine angularity to a male face.
Modifying these elements in ways that magnify attention on the eyes and lips gets at the heart of optimization.
3. What are the indications for facelift surgery in those who aren’t yet showing classic signs of age?
[See Figures 1 and 2 below]
In younger patients and for those who aren’t showing classic signs of age, the indication for an optimization facelift is a bottom-heavy appearing face. While often mistaken for premature aging, the real driver often is inadequately projecting bone structure — here, the skeletal framework can’t support tissues and drooping creates a sagging, pseudo-aging appearance. In this situation, we first need to enhance the underlying framework so that a facelift can be effective and last. On the other hand, a facelift done on an unsupported frame is like hanging a heavy ballgown on a thin hanger — it’s destined to slide off. So my strategy first is to optimize bone structural support by augmenting the midface, and deep plane face and neck lift to reposition tissues on a strong foundation. This can often be done safely in 1 surgery.
4. Beyond recontouring the jawline/neck, how are you able to make a face look objectively prettier with surgery?
Ultimately, beautification should bring more of the observer’s attention to the eyes and lips (which form the “triangle of Yarbus” — in the 1960s, Yarbus proved through eye tracking that the human gaze is focused on eyes and lips). To do this, I use “direct” and “indirect” methods to bring more attention there. “Direct” modification of the eyelids often involves lower blepharoplasty and fat grafting to correct under eye bags, while orbital rim (eye socket bone) implants can smooth deep tear troughs, boost the lower eyelid and correct eye shape and position. Lateral eyelid corner release and lifting through canthoplasty elongates and upwardly tilts the eyes, while endoscopic brow lift brightens eyes by lifting drooped eyelid skin. For the lips, fat grafting and upper lip lifts can increase volume and “neotenize” them.
For women, “indirect” methods involve reducing the nose and facial frame, whereas for men I often augment and/or define, rather than reduce, these areas. Forehead reduction (lowering the hairline) and “V-line” jaw and chin slimming make the face smaller so eyes and lips appear relatively larger in size —an indirect effect. Reduction rhinoplasty both neotenizes the nose and also makes it less distracting from the eyes and lips — another indirect effect. Narrowing nasal width can also create an optical illusion that the inter-ocular space (i.e., distance between the eyes) is elongated which can also beautify the eyes (eg., Daphne Groeneveld or Yael Shelby — note their eyes are slightly wider apart). These maneuvers are subtle yet synergize to make the eyes and lips appear relatively larger by proportion with the smaller facial frame.
Finally, deep plane facelift and deep structural necklift repositions facial and neck tissues to optimize the midface-to-lower Ogee curve and to reveal optimized jawbone structure. I often do these as a final step because face and neck lift is more effective when the facial architecture is optimized.
5. What’s generally the age range for these patients? What’s the youngest “beautification” type lift you’ve done?
The age range is generally mid-30s to mid-40s, and the youngest patient I’ve treated with full face optimization is 29 (see Figures 1 and 2).
6. When do you say no to a facelift on a younger person?
Since beautification is about anatomy, age is not the sole determinant of suitability for surgery. Be that as it may, in a broader context of ethics and patient safety, proper patient selection is crucial and I turn away patients whose goals are unrealistic or dangerous or who have body dysmorphia.
Social media has distorted the perception of beauty to extremes and so I weigh carefully patients’ emotional and psychological fitness to undergo significant surgery. With all patients, I always solicit input from their medical doctors and specialists (including psychiatrists when appropriate) to ensure that patients understand the gravity of the undertaking, permanence of change, and risk/reward balance.
7. When the goal is to beautify rather than anti-age, do you approach the surgery itself differently? Are there technical differences?
Yes, when the goal is to beautify or optimize, there are differences in both procedure selection and surgical technique:
1. With respect to procedure selection, in optimization I routinely modify the facial skeleton with high-density porous polyethylene (HDPPE) implants to enhance midface bone structure and make eyes appear more deep set. Also, V-line jaw and chin slimming for women, and chin and jaw augmentation for men, rebalance the facial frame. These are much more common in optimization than rejuvenation.
2. Also, there are technical differences: in optimization, I elongate and lift brows more horizontally and slightly vertically with a goal of brightening eyes, whereas in rejuvenation, brows are more lifted vertically than horizontally with minimal change in eyelid shape. Beautified eyes tend to be slightly tilted and elongated and sometimes this requires a “bone anchor” method of canthoplasty (outer eye corner lift) whereas in rejuvenation I may release the outer eye corner but usually don’t employ bone anchoring. Rejuvenation rhinoplasty is focused on correcting age-related tip droop and bulbosity, whereas optimization focuses on overall size reduction (for women), tip definition and bridge contour improvement.
However, there is overlap in procedure selection between optimization and rejuvenation, for example upper lip lift and fat grafting can be used in either scenario though with different goals and technique.
8. Is the recovery generally the same?
Typically yes. Pain is not a major factor in recovery, whereas swelling typically lasts a few weeks before faces appear normal to others. This is generally the same between optimization and rejuvenation, although when more procedures or bone contouring work is involved it can take a bit longer.
9. When someone has a facelift on the younger side, how does it change the trajectory of aging?
Optimized faces often have enhanced bone structure — this provides better support to soft tissues which changes the trajectory of aging more favorably. Unlike a rejuvenating facelift which corrects signs of aging, beautification is about optimizing facial aesthetics though it often has a secondary impact on aging because better facial architecture slows age-related tissue descent. While many genetic and environmental factors are at play in the arc of aging, better bone structure generally translates to more graceful aging.
10. Many plastic surgery procedures are done solely to enhance the appearance rather than repair or restore, but the facelift has always been associated with aging and reserved for older patients. What factors are contributing to the rise of the beautification lift?
Due to a step-change in surgical techniques in recent decades that focuses on deeper anatomical structures, the paradigm has shifted from facelifts as late-stage restorative procedures to earlier structural interventions aimed at aesthetic optimization. Younger patients are increasingly seeking contour enhancement and proportion correction without the volumization of injectable fillers, and often in the absence of significant tissue droop. This demand is driven by greater aesthetic literacy, visual self-scrutiny via high-resolution imagery, and disillusionment with the volumetric distortion of repetitive filler use.
Patients are realizing that facial optimization isn’t about looking younger—it’s about looking better. They’re seeing that subtle, well-planned surgical refinement done early can look more natural and elegant than years of overfilling or chasing trends. As surgeons, we must approach these cases with heightened restraint and artistic precision especially since the margin for error is narrower, and the goal is subtle elevation rather than restoration.
As an aside, the term “facelift” is a misnomer in face optimization since it conjures the notion of lifting back up that which has fallen — an aging concept. Face optimization may or may not employ a facelift, but more accurately it is a sculptural approach.
11. What kind of feedback do you get from “beautification” patients versus those who get lifts later in age/for more conventional reasons?
Both groups — beautification and rejuvenation — often describe feeling more confident and aligned with how they imagined they could look. But the origin of that confidence is different: in rejuvenation, patients are more confident having recaptured a prior appearance whereas beautification patients feel empowered with a fresher look they’ve never experienced before. Both are powerful, but for different reasons.
12. Where’s the line between a beautification facelift and a traditional facelift (I’m guessing even some of your younger patients might have some signs of early laxity)?
Yes, the line is blurred because it isn’t strictly about age—it’s about intent. A traditional facelift aims to restore what has faded through aging, while a beautification facelift builds on what may have never been there to begin with: sharper angles, better proportions, more facial harmony. That said, even younger patients often show early signs of laxity—so the approach becomes hybridized. I’m not just lifting to turn back time — I’m sculpting to elevate the face toward its ideal, often correcting congenital or structural imbalances along the way. Overall, I believe that best results are achieved with millimeter changes in many areas throughout the face.
13. Over the past year, we’ve heard a lot about the “glow-up” facelift, with much celebrity speculation. Do you think it’s risky to equate a facelift with a “glow-up”?
The “glow-up” facelift is catchy, but also a bit misleading. If by ‘glow-up’ we mean refined, natural, sculptural improvement that enhances confidence—then yes, that’s absolutely possible with the right technique, and can be achieved non-surgically in some cases. When a facelift is associated with a quick fix or viral transformation, that’s where it gets risky as it trivializes the artistry and responsibility of surgery. Surgery isn’t a filter. A facelift is a serious, permanent intervention that demands keen judgment, technical artistry, and safety as a priority. Equating it with a trending term can minimize the complexity and lead to unrealistic expectations. A true glow-up doesn’t come from chasing someone else’s face. Rather, it comes from elevating your own features with precision and purpose.
14. The WSJ recently reported on facelifts at 35. Five years ago, we were writing about facelifts in the 40s. Where is this trend headed?
We used to talk about facelifts in the 50s, then 40s—and now 30s. But it’s not about age—it’s about anatomy, goals and intention. I think we’ll see more patients seeking structural solutions earlier, not because they look older, but because they want to look better in ways that give lasting, natural results. And modern surgical approaches can offer tremendous nuance never before possible.
15. Do you see this as being a sort of slippery slope for surgeons? I’m sure you want to offer the most effective treatment, regardless of a patient’s age, while also being careful not to position the facelift as a sort of cure-all for everyone.
Absolutely. Just because someone can technically have a facelift doesn’t mean they should. The surgeon’s role is to guide, not enable. My philosophy is simple: do the right procedure, for the right patient, at the right time. And sometimes that means saying no.
**
Jessica’s story
See accompanying Figures 1 and 2 below.
In the years before her surgeries with me, Jessica was concerned about early signs of aging including hollowing of her under eyes, drooping cheeks, and downturned eyes and mouth corners that she felt conveyed an aged appearance beyond her years. Initially she underwent injectable filler treatments, but quickly experienced their limitations: in addition to the temporary effect of fillers, she developed “filler fatigue” with progressive and unnatural inflation of her features after successive treatments. She felt as though she was becoming unrecognizable and wanted to restore natural proportions, optimize her facial features, and lift with permanent effects.
Although a facelift factored into my surgical plan, the overarching question was why her face was dropping faster than her age would predict? Diagnosing root cause is always my priority in order to arrive at the optimal surgical approach, and in examining her facial architecture it was immediately clear to me that she lacked optimal mid-facial bone structure from her lower eye sockets to outer cheekbones, areas which are critical for aesthetic proportions and tissue support. This is what led to her premature under eye hollowing, drooped eye corners and a bottom heavy lower face and neck. Therefore, enhancing her facial bone architecture was essential both for the aesthetic improvements she desired and also for longevity of her facelift.
First she had fillers dissolved, and then I planned a two staged surgical approach, first with a forehead reduction, fat grafting and buccal fat reduction for better facial proportions, and also implants made of high-density porous polyethylene (HDPPE), a biocompatible, lightweight bone-like material, to augment her lower eye socket and cheek bones. These implants gave a strong foundation to support repositioned facial fat from a deep plane face and neck lift in the second stage. Additionally, reversing the downward tilt to her eyes with “canthoplasty,” a delicate lift of the outer eye corners, along with an upper lip lift and fat grafting, completed the second stage and her overall results which are shown at 15 months after her second surgery.
Figure 1:

Figure 2:

Prescott’s story (see Figures 1 and 2 below)
Prescott wanted to look more attractive though he didn’t know how to articulate his goals. He produced a picture of a male model with chiseled features, high arched cheekbones, deep set eyes and a straight nose — the opposite of Prescott’s features. The problem was not the soft tissue or aging, but rather his underlying facial architecture. It became clear that we needed to reshape the framework in order for the tissues to drape more aesthetically. Prescott lacked optimal mid-facial bone structure which created a bulging eye appearance, under eye bags, deep tear troughs, bulging lower cheeks and concave appearance face. Like Jessica, enhancing his facial bone architecture was essential both for the aesthetic improvements and after consulting several times, he and I decided to proceed in 2 stages.
First stage of surgery focused on the skeletal foundation of his midface, and I placed porous polyethylene implants over the lower eye socket and central maxillary bone, corrected under eye bags with lower blepharoplasty, smoothed lid-cheek junction and enhanced high arched cheekbones with fat grafting, and de-volumized the lower cheek fullness with buccal fat reduction. About 1 year later, with optimized facial architecture, in the second stage I improved his nose with closed rhinoplasty, and sharpened his jawline with deep structural necklift. Note that no traditional facelifting was done.
At 2.5 years after surgery he looks more attractive and masculine owing to deeper set eyes, supported lower eyelids, an aesthetically optimized midface Ogee curve (convex upper midface to concave lower cheek), a straight and defined nose, and defined jawline.
Figure 3:
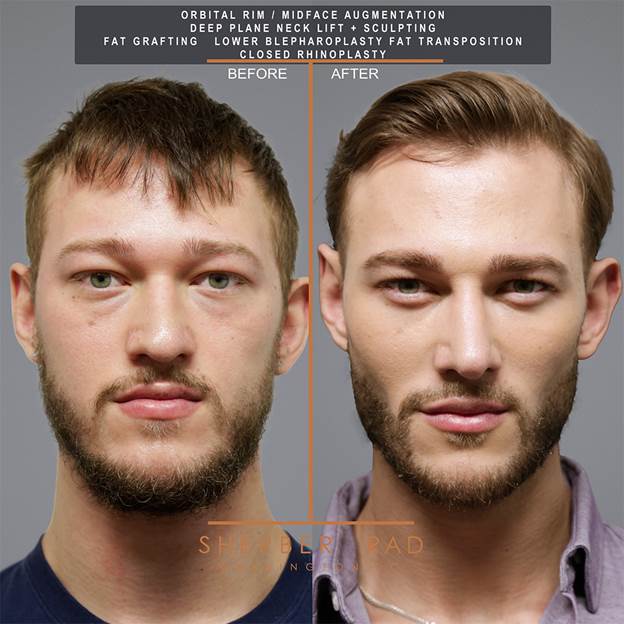
Figure 4:
